Use of Abdominal Adipose Tissue for Interposition in Unilateral Temporo-Mandibular Joint Ankylosis - A Case Report
<p style="text-align: justify;">Introduction: Temporo-mandibular ankylosis is a debilitating condition resulting in immobile lower jaw, reduced mouth opening, facial asymmetry and reduced general health status. This article is a case report of post traumatic unilateral TMJ ankylosis in a young female treated successfully by surgery wherein the abdominal adipose tissue with dermis was used for interposition to prevent reankylosis.</p> <p style="text-align: justify;">Case Report: A female patient twenty two years old diagnosed as unilateral TMJ ankylosis. The surgical treatment of gap-arthoplasty with inter-positional grafting with abdominal fat pad and bilateral coronoidotomy was planned</p> <p style="text-align: justify;">Discussion: The success in the preventing Reankylosis after TMJ gap arthroplasty is related primarily to the appropriate surgical technique with adequate removal of bone, early vigorous postoperative physiotherapy, maintained for long term. The case reported has no obvious facial deformity, one stage treatment of release of ankylosis and interposition of abdominal fat has improved patients mouth opening. The ease of harvesting and sufficient size of tissue definitely makes abdominal derma fat as choice of interpositional autogenous tissue in case of TMJ ankylosis.</p> <p style="text-align: justify;">Conclusion: The results obtained in our study are highly satisfactory and encouraging, supporting the role of abdominal dermis fat graft as the interposition material in TMJ Ankylosis cases. However, a large sample size and a longer follow-up period are required to consolidate the findings.</p>
Jhon4 and Sujit Wyawhare4
Varsha_manekar@yahoo.co.in
for interposition to prevent reankylosis.
abdominal derma fat as choice of interpositional autogenous tissue in case of TMJ ankylosis.
Conclusion: The results obtained in our study are highly satisfactory and encouraging, supporting the role of abdominal dermis fat graft as the interposition material in TMJ Ankylosis cases. However, a large sample size and a longer follow-up period are required to consolidate the findings.
Keywords: Abdominal Adipose Tissue; Temporo-Mandibular; Intracapsular Condylar; Glenoid Fossa; Coronoid.
Introduction
Temporo-mandibular ankylosis is a debilitating condition resulting in immobile lower jaw, reduced mouth opening, facial asymmetry and reduced general health status. Management of ankylosis occurs through surgical intervention; several authors agree that it is necessary to use an interpositional material to prevent re-ankylosis after gap arthroplasty. The primary function of the interpositional material is to prevent the reankylosis by eliminating contact between bone surfaces. Appropriate inter positional material include: 1-autogenous tissue: meniscus, muscle, fascia, skin, cartilage, fat or combination of these tissues; 2: allogeneic tissues; cartilage and dura; 3; alloplastic: silastic materials like acrylic, proplast, and silicon; 4: xenograft tissues: usually of bovine origin (collagen and cartilage). The prevalence of ankylosis as given by one study conducted in India is 0.46 per 1000 population in the 3-15 years of age group. The etiology in this age group is forceps delivery or ear infection. In the older population the commonest reason is trauma. The intracapsular condylar fracture if not treated properly the ankylosis of TMJ (Temporo-mandibular joint) results. This article is a case report of post traumatic unilateral TMJ ankylosis in a young female treated successfully by surgery at our department wherein the abdominal adipose tissue with dermis was used for interposition to prevent reankylosis.
Case Report
A female patient twenty two years old reported with complaint of inability to open mouth since 10 years. She gave history of trauma and mandibular fracture twelve years back. The mouth opening gradually reduced since then. The general condition was fairly good. The face appeared asymmetric with fullness on left side, & flattening oh right side of face. The mouth opening of only seven mm as seen in Figure 1. The condylar movements on right side was diminished and no movement on left side. The occlusion was deranged with midline shift. The Orthopentamogram (OPG) shows (Figure 2) normal right condyle. The left condyle had wide neck and a bony chunk between glenoid fossa and ramus. The coronoid process appeared elongated. The case was diagnosed as unilateral ankylosis of TMJ. The lateral view for evaluation of the pharyngeal airway was done, it was sufficient. The CT scan images figure 3 shows loss of architectural morphology of left mandibular condyle and temporal fossa showing moderate amount of new bone formation, articular surface irregularity, erosion along left condyle and articular eminence with significantly reduced TMJ space.



Figure 3: Preoperative CT scan images. The case was diagnosed as unilateral TMJ ankylosis. The surgical treatment of gap-arthoplasty with inter- positional grafting with abdominal fat pad and bilateral coronoidotomy was planned. The necessary blood investigations were done. The patient was taken under general anaesthesia with fibreoptic intubation maintained on hypotensive anaesthesia. The alkayat- bramley incision was taken for approaching the ankylosed mass in temromandibular region as seen. The skin & superficial fascia flap reflected to expose the pre auricular TMJ region. The oblique incision taken on the zygomatic arch and the subperiosteal dissection done to expose the ankylotic mass as seen in figure 4. A complete bony union of glenoid fossa in sphenoid bone and the superior part of ramus was seen. A condylar retractor was positioned and gap arthoplasty performed. Figure 5 shows the gap created of 1.5mm. The smooth surface on medial side was confirmed as remnant of head of the condyle displaced in previous fracture. The ipsilateral coronoidectomy was performed through same surgical approach. The contra lateral coronoidotomy was performed intraorally. The mouth opening achieved after this was 45mm as seen in figure 6.
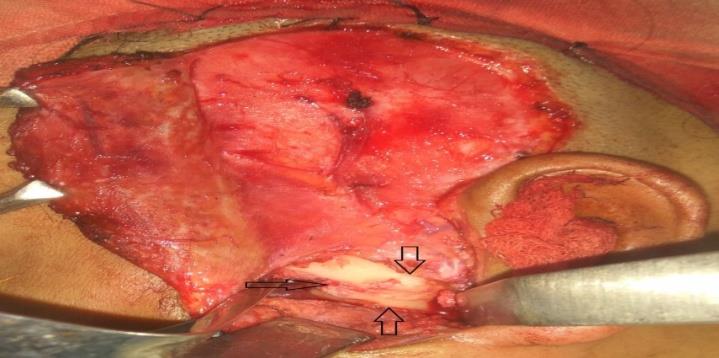
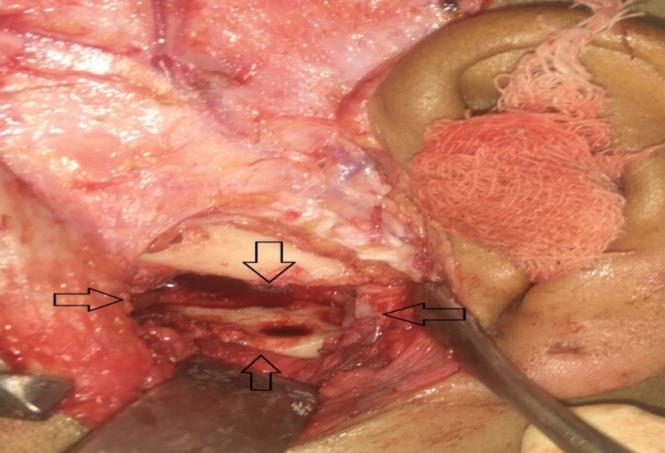


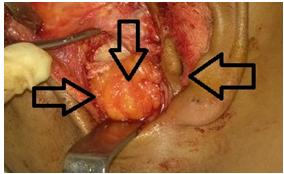

Figure 9: Postop OPG. This acts like interposition to prevent reankylosis. The layer wise closure with interrupted suturing and mini vac drain placement was done. The patient was extubated and post anaesthetic recovery was uneventful. The patient was kept on forceful mouth exercise under supervision with Heister’s mouth opener. Figure 9 shows the post operative OPG showing the gap in place of TMJ. She was guided to close with elastics. The mouth opening maintained was 29mm after one month. She is still under long term follow up.
Discussion
The above reported case as seen from imaging is type IIISawhney classification. These cases are difficult for intubation for anaesthetists. The Tracheostomy was planned as alternative in case of inability of nasal intubation. Our senior anaesthetists performed fibreoptic intubation successfully which avoided the need of tracheostomy in our patient. The traditional approach of TMJ ankylosis is by gap arthoplasty. Gap arthoplasty is procedure for release of the ankylosed joint, removal of the heterotopic and reactive bone with thorough debridement (gap arthroplasty of at least 2.0–2.5 cm). The first reported use of autologous fat graft placement into the TMJ for the treatment of ankylosis was by Blair in 1913 followed by Murphy in 1914 [1, 2]. Till 1990 there are no references in literature. In 1992, Wolford developed the technique of placing autogenous fat grafts around the TMJ Concepts to prevent postsurgical heterotopic bone and fibrosis development (In their article on management of TMJ ankylosis [3]. Movahedand Mercuri, mentioned the rationale for placing autologous fat grafts around the TMjoint replacement was to obliterate the dead space around the joint prosthesis, thus preventing the formation and subsequent organization of a blood clot [4]. According to Movahedand Mercuri creating this physical barrier serves to minimize the presence of pluripotential cells, and prevents the formation of extensive fibrosis and heterotopic calcification. The fat grafts may be inhibitory to heterotopic bone formation. Dennis J Kantanen discussed the use of abdominal fat harvest and augmentation in maxillofacial surgery [5]. They described it as relatively inexpensive, safe, and readily available. The uses of derma fat minimize the fibrosis and bone formation in TMJ ankylosis. Kaufman, et al. found that fat transferred into subcutaneous tissue demonstrated 30% survival after 6 months [6]. Keerl, et al. studied fat implanted into the frontal sinus of 11 patients for obliteration of the frontal sinus cavity [7]. Postoperative magnetic resonance imaging evaluation showed viable fat in 6 of the II patients 4-24 months after surgery. In the remaining 5 patients, the fat demonstrated necrosis and had been replaced by granulation tissue and connective tissue. The abdominal fat harvesting is considered to be a safe procedure with minimum morbidity. The possible problems mentioned are seroma, infection, hematoma, ileus, and inadvertent peritoneal perforation [4]. The incidence of 6.9% of seroma formation requiring aspiration is reported by Wolford et al. postsurgical abdominal seromas are typically evacuated with percutaneous drainage and aspiration under local anesthesia. Infection rates are consistent with any other surgical procedure, with an incidence of around 3%. Abdominal subcutaneous hematoma formation is a rare occurrence during abdominal fat harvest, with a reported incidence between 0% and 3.2%, owing to the small surgical field, short surgical time, and ease to obtain hemostatis. With careful attention to hemostasis, drain placement into the harvest site is rarely needed. Adequate
placement of fluffed gauze and elastic dressing minimizes the incidence of hematoma formation. Postsurgical ileus and inadvertent peritoneal perforation are possible sequelae during abdominal fat harvest. The temporalis fascia with muscle is routinely used for interposition in the gap after release of TMJ ankylosis. The adjacent donor site, ease of harvesting and good blood supply makes it a good choice. The drawback observed is the trismus developed postoperatively causes difficulty in maintaining the mouth opening achieved postoperatively and occasional hematoma formation. Difficulty in mouth opening and vigorous post operative exercise are troublesome for the patient if Temporalis muscle is used as the interposition material due to compression of the nerves which may subsequently reduce the mouth opening. An ugly bulging in the temporal region after harvesting of that side may not be neglected. However the versatility of the Temporalis Myofacial flap technique in Interpositional material is not certain and failure may occur. The jaw movements and physiotherapy are well tolerated and maintained by patients if the gaps were filled with dermis fat grafts. The dermis fat graft minimizes the occurrence of excessive joint fibrosis and heterotopic calcification and consequently providing improved range of motion. Graft procurement is quick and easy with minimal morbidity and the wound and scar in the anatomical skin creases are accepted cosmetically. The case reported has no obvious facial deformity, one stage treatment of release of ankylosis and interposition of abdominal fat has improved patients mouth opening. The ease of harvesting and sufficient size of tissue definitely makes abdominal derma fat as choice of interpositional autogenous tissue in case of TMJ ankylosis. The case need follow up for long time.
Conclusion
The success in the preventing Reankylosis after TMJ gap arthroplasty is related primarily to the appropriate surgical technique with adequate removal of bone, early vigorous postoperative physiotherapy, maintained for long term.
The results obtained in our study are highly satisfactory and encouraging, supporting the role of abdominal dermis fat graft as the interposition material in TMJ Ankylosis cases. However, a large sample size and a longer follow-up period are required to consolidate the findings.
References
-
Blair VP (1913) Operative treatment of ankylosis of the mandible. Trans South Surg Assoc 28: 435-463.
-
Murphy JB (1914) Arthroplasty for intra-articular bony and fibrous ankylosis of the temporomandibular articulation. J Am Med Assoc 62(23): 1783.
-
Wolford LM, Morales Ryan CA, Morales PG, Cassano OS (2008) Autologous fat grafts placed around temporomandibular joint total joint prostheses to prevent heterotopic bone fonnatioo. Proc (Baylor Univ Moo Cent) 21(3): 248-254.
-
Movahed R, Mercuri LG (2015) Management of temporomandibular joint ankylosis. Oral Maxillofacial Surg Clin N Am 27(1): 27-35.
-
Kantanen DJ, Closmann JJ, Rowshan HH (2010) Abdominal fat harvest technique and its uses in maxillofacial surgery. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 109(3): 367-371.
-
Kaufman MR, Bradley JP, Dickioson B, He Uer JB, Wasson K, et al. (2007) Autologous fat transfer national consensus survey: trends in techniques for harvest, preparation, and application, and perception of short- and long-term results. Plast Reconstr Surg 119(1): 323-231.
-
Keerl R, Weber R, Kable G, Drat W, Constantinidis J, et al. (1995) Magnetic resonance imaging after frontal sinus surgery with fat obliteration. J Laryngol Otol 109(11): 1115-1119.
- Psychogenic Erectile Dysfunction in Late Adulthood: A Case Report on Clinical Intervention and Intimacy Restoration
- Clinical Trials on COVID-19 in 2025: A New Chapter in Global Health Research
- Innovations and Challenges in Contemporary Medical Clinical Trials: An Editorial Perspective
- Innovations and Challenges in Contemporary Medical Clinical Trials: A Critical Perspective
- Reimagining Clinical Trials: The Power of Continuous Feedback from Medical Reports
- Factors Influencing Brain Drain: Perspectives from a Medical School in Turkey